
Breast Augmentation
Breast Augmentation
Breast augmentation is a surgical procedure that enhances the volume and shape of the breast, either after loss of fullness from breastfeeding and weight loss, or limited development at puberty. This is accomplished by insertion of medical devices called breast implants.
There are different types of breast implants available, as well as different surgical approaches. There is not one implant or approach that is best for every augmentation. Breasts are extremely different, even from one side to the other, and different approaches will give better results in different breasts.
What kinds of implants are available?

Implants can be categorized according to their fill and surface of the shell.
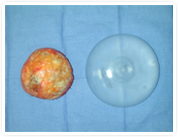
Saline implants have the same type of silicone elastomer shell as silicone implants do. The saline implant shell comes out of the package uninflated and is filled with sterile, injectable saline (the same salt water that goes in an IV) at the time of surgery (see left). Even though there are different sizes of implants available, each size can be under- or overfilled to a desired volume to a certain extent. Wrinkling is more prominent with saline implants than with silicone. If a saline implant were to rupture, you would know right away as the implant deflates and the fluid is absorbed into the bloodstream, leaving the body in your urine.
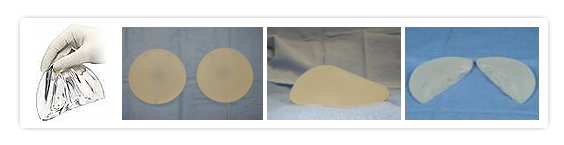
Silicone implants are filled with a gel of cohesive silicone that makes the implant feel softer than saline implants. The amount of chemical crosslinking within the gel makes the consistency softer or firmer. The “gummy bear” implant (one of which has been cut and shown above) is a type of silicone implant that is firmer due to more crosslinking and therefore able to be made into a shaped, or anatomic, implant. Wrinkling is less prominent in silicone implants than in saline implants, but can still be a potential problem in patients with very thin soft tissue to cover the implant. With the current generation of silicone implants available, the rupture rate is much less. When it does occur, the gel simply stays in place either within the shell or capsule around the implant.
The U.S. Food and Drug Administration (FDA) placed silicone implants on a moratorium in 1992 to review complaints from patients that silicone was related to a group of disorders called connective tissue diseases. Based on all the scientific studies and careful independent review by the National Academy of Sciences Institute of Medicine, the FDA determined that there is NO link between silicone and any adverse health risks, and decided to make silicone implants available again to the general public in 2006.
There are smooth and textured surfaces of the implant shell, whether the implant is filled with saline or silicone. Smooth shells allow the implant to move around freely in the pocket, or capsule, that is formed by your body. Textured surfaces are meant to encourage “tissue ingrowth” by your body so that the implant will tend to stay in one place. The shaped, or anatomic, implants all have textured surfaces so that the implant will not rotate. Some surgeons believe texture protects against capsular contracture, but the adherence to your soft tissues may also make wrinkling more visible.
What happens at my visit?
At your consultation, Dr. Huang will complete a thorough examination, taking measurements of your breast and determining its proportion to the rest of your body. She will also discuss your preferences regarding breast size, incision location, and most importantly, exactly how you would like your breast to look.
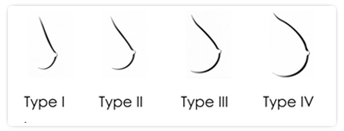
Results can be classified into four types.
- A Type I result is slightly scooped out at the top and does not fill the skin envelope completely.
- Type II fills the skin envelope proportionately, and would not be known to be an augmentation to observers.
- A Type III result has a more rounded appearance, particularly at the top of the breast, which would be visible in clothes.
- A Type IV result is an obviously augmented breast.
The degree of skin stretch you have of the breast (the “skin envelope”) will determine how much volume it will accommodate. Often women want to achieve more cleavage. This depends on the position of your breasts on your chest wall. Even with a significant breast augmentation, it is possible that you would be unable to have cleavage.
Differences often exist between your breasts, in size, position on the chest wall, and even nipple location. After breast augmentation, these differences will remain, and in some cases may even be exaggerated. Rest assured that Dr. Huang does everything she possibly can to minimize such differences, or asymmetry. Also, if you are predisposed to stretch marks and prominent veins, these may become more marked after surgery.
After examining you and discussing your desires, Dr. Huang will recommend a range of options for implant type and size that will best suit your breast and balance with the rest of your figure. She will always honor your choices of alternatives if she feels she can achieve an aesthetic breast using your choices.
Where does the implant go?
Covered by the skin and subcutaneous fat, the breast gland itself sits on top of the pectoralis major muscle. The muscle has a fibrous covering called fascia. The breast implant can be placed directly under the breast gland (“subglandular”), under the pectoralis major muscle (“subpectoral” or “submuscular”), or under the fascia of the pectoralis major muscle (“subfascial”).
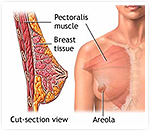
The subglandular pocket provides the most natural result of all because it allows the implant to “fall” with gravity, providing a “natural” breast shape. It also allows for “cleavage” if your breasts already meet in the middle naturally. Some surgeons shy away from this pocket because of the risk of capsular contracture, which will be discussed later.
Subpectoral or submuscular placement is necessary when the tissue thickness of the skin and soft tissues are not sufficient to camouflage the borders of the implant. Some surgeons feel that the subpectoral pocket minimizes capsular contracture. The trade-off for avoiding this complication is an “animation deformity,” where the implant moves from the action of the pectoralis muscle.
The subfascial approach is a more recent development that theoretically combines the advantages of each of the above pockets. The merit of this technique has not yet been clearly established.
How is the implant put in?
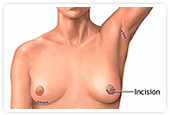
Most commonly, the implant is placed through incisions either in the breast fold, (“inframammary”), along the border of the areola (“periareolar”), or in the armpit (“transaxillary”).
The traditional incision is through the inframammary fold, under the breast. While this is an incision directly under the breast, it is the least visible as it is hidden underneath the projecting pole of the breast. This approach allows for the best visualization for the surgeon, and is often the incision of choice anytime a revision is necessary. It is also the most common incision choice for placement of the anatomic implants.
The periareolar incision is a half circle incision along the lower border of the areola, or pigmented skin around the nipple. This incision stays fairly well hidden, but may not be an option for patients with a naturally small areola because it will not be large enough to insert a silicone implant. A saline implant would be possible in such a case because it is deflated at the time of insertion. This incision is also a good approach especially when an implant is being placed in conjunction with a breast lift.
An incision can be placed under the arm in the hollow of the armpit, called the transaxillary incision. This approach avoids any scars on the breast itself. If reoperation is required, however, an inframammary incision most likely will be necessary.
Finally, the transumbilical approach uses an incision just above the belly button, similar to a laparoscopic incision. Tunnels are made through the soft tissue of the upper abdomen to the breast. Due to the nature of the technique, silicone implants of any type cannot be used with this technique. Again, if any complications were to occur, then an inframammary incision would be necessary. Of note, breast implants have not been approved by the FDA for insertion through the transumbilical approach.
What is involved in the operation and how long will I be off work?
Breast augmentation is an outpatient procedure that we perform at the Los Robles Surgicenter, Specialty Surgical Center in Westlake, or Thousand Oaks Surgical Hospital. The procedure itself can take from 1-2 hours, while you are asleep under general anesthesia. You can expect swelling and possibly some bruising for 3-10 days. Having implants placed under the muscle does cause more discomfort initially than having them placed subglandularly.
Depending on your type of work, you should be able to return to work and social activities within 3-5 days. Any aerobic exercise that will elevate blood pressure or heart rate is not allowed for 4 weeks after surgery regardless of the technique performed. Driving is allowed once you feel well enough to be able to turn the steering wheel suddenly and forcefully if necessary.
Is this procedure safe?
Breast augmentation is an elective procedure. Any surgery is a stress to your body, and the inherent risks of infection, bleeding, delayed healing, and risks of general anesthesia exist. As for the implants themselves, as mentioned before, silicone has been proven not to be associated with the development of connective tissue disease.
What if I have children after augmentation? Will I be able to breastfeed? Will my children be affected?
In all approaches, the breast tissue itself is minimally disrupted and thus should not interfere with breast feeding. Keep in mind that there are some people that are unable to breastfeed, even before undergoing surgery. It may be possible that you will require formula supplementation in addition to your own breast milk.
Some have expressed concern about the safety of breastfeeding with silicone implants in. Multiple studies have confirmed that silicon levels (a marker for silicone) of women with silicone implants in blood and breast milk have not been significantly higher than those of the general population. In fact, silicon levels in cow’s milk are more than a few hundred times higher and levels in infant formula thousands higher than in breast milk.
Several large studies have shown that children of women who have had breast implants are not at higher risk for any health conditions.
What exactly are the concerns about silicone?
In 1992, the FDA took silicone implants off the market because a number of complaints of implants being associated with a group of disorders called connective tissue diseases, or autoimmune diseases. These conditions involve the body essentially attacking itself by way of its own immune system. After thorough independent review by the National Academy of Sciences Institute of Medicine, and independent statements by the American College of Rheumatology and the American Academy of Neurology, it was determined that there is no scientific evidence to demonstrate an association between silicone implants and systemic autoimmune or neurologic diseases. As a result, silicone implants were made available to the general public again in 2006.
Furthermore, breast implants do NOT cause breast cancer, nor do they weaken the immune system. What is true is that silicone is in direct contact with the adjacent breast tissue and can be found in the capsule tissue that the body forms around the implant, whether the implant is filled with saline or silicone.
The concerns you should have regarding silicone implants are the body’s local reaction to having the foreign bodies placed within you. Depending on the severity, these reactions may require additional surgeries for you. Statistics show that a large number of women could expect to have an additional procedure within 5 years of their initial surgery.
When would I require additional surgery?
Hematoma
An important complication that requires an additional surgery is the development of a hematoma, which is a collection of blood. At the time of surgery, dissection through blood vessels is controlled by cauterizing the cut ends of the vessels. Sometimes, after a patient has gone home, a transient increase in blood pressure or sudden movement may cause the clot to dislodge, thereby allowing for active bleeding. This is a surgical EMERGENCY which requires immediate attention to stop the bleeding. Symptoms would include increasing pain, enlargement of the affected side, and change from a soft breast to a firm hard mass.
Infection
Anytime a “foreign body” is in the body, there is a risk for infection. Infections occur most often in revisional surgery. Sometimes it is a simple infection that causes redness or swelling, which may require antibiotics. Intravenous antibiotics or a hospital admission may be necessary in more severe cases in an effort to save the implant. In the most severe situations, the implant may need to be removed and the tissues allowed to settle over 6 months before an implant is reinserted.
Implant Replacement
It is important to recognize that most women will “outlive” their implants. The current generation of implants is much more resistant to rupture than the previous generation, which required replacement at 10-15 years. However, barring any other complications, their longevity is yet unknown.
Implant Rupture
How does an implant rupture? Wrinkling is inherent as the implant settles with gravity, which may be visible in some thin patients. With time, the repetitive rubbing of the implant wall will create “fold flaws,” which are weakened, thinned areas in the implant wall. As the wall weakens, any trauma such as a car accident to even a routine mammogram can be enough force to facilitate an impending rupture. Saline implants simply deflate when ruptured. If a silicone implant ruptures, the gel will remain within the capsule. If the capsule tears from a traumatic event, the immune system may react to the now “free gel” by forming either granulomas, evidenced as lumps, or enlarging lymph nodes in the axilla. For these reasons, any rupture of the implant, even a “silent rupture” that is not bothering you, requires another surgery to either replace or remove the implant. Even if one side is affected, sometimes it is beneficial to replace or remove both sides to maintain symmetry (evenness). As a result, the implant companies require MRI surveillance of silicone filled implants starting at 3 years after your initial surgery, and every other year thereafter. There may be additional costs involved for the MRIs.
Capsular Contracture
Capsular contracture remains the most puzzling and, unfortunately, the most common complication of breast augmentation that requires further surgery. The body’s normal response to finding a “foreign body” is to “wall it off” with scar tissue, which forms a capsule. This capsule is fine and normal as long as it stays soft. Sometimes, the scar tissue continues to build and build until it thickens and subsequently squeezes down on the implant, distorting the shape. This creates a deformity of the breast, either by forcing the implant to a higher position on the chest wall, or simply distorting the shape of the breast itself. It becomes quite firm and is sometimes accompanied by severe pain as well. There are many theories and studies investigating the source of this phenomenon, but there are no good, proven ways of preventing capsular contracture. There are some medications used for asthma and circulatory problems that have been shown to provide some relief, but these are not without side effects themselves. The current solution is simply to cut out the scar tissue at another surgery and reinsert the implant.
Known factors associated with higher rates of capsular contracture are the use of smooth surfaced implants and the subglandular pocket. Even though the subpectoral rate may be lower, this rate must be weighed against the development of an animation deformity. Capsular contracture does occur in the subpectoral and subfascial planes as well, but may be better tolerated due to the increased amount of tissue covering and camouflaging the implant.
Animation deformity
Animation deformities, as mentioned before, occur because the pectoralis major muscle is now wrapped around the top of the breast implant. With movement of the shoulders, the muscle still contracts and now transfers some of its action to the implant, causing it to move around in its pocket. In addition, following augmentation, the pectoralis muscle fibers can sometimes reattach by way of scarring to the overlying skin and also pull the skin and breast tissue with each contraction, causing significant shape changes with movement. Although not medically necessary, some women are not able to accept this deformity and require a pocket change to remove the effect of the muscle.
Implant related concerns—size change, wrinkling
Lastly, many reoperations are performed for cosmetic reasons, most commonly for a size change. In most cases, there will be additional costs of surgery for use of the facility and anesthesia. It is also important to check with your insurance company as many now specifically exclude coverage of any implant related procedures or complications.
What about breast cancer?
This is a very important question you must consider. Breast implants do NOT increase the chance of cancer. Even so, 1 in 8 women today will develop breast cancer sometime in their lifetime. You must understand the implications of having breast implants in the process of breast cancer screening, diagnosis, and treatment.
Mammography is still the best mode of screening for women with breast implants. With implants, technicians will need to displace (move) your implants and take extra views (not significant, but added radiation) to better visualize your breast tissue. Implants WILL decrease the amount of breast tissue that can be seen by a radiologist, the degree of which depends on whether the implants are subglandular or subpectoral, and whether or not you have capsular contracture. Subpectoral implants interfere least with visualization as long as there is no capsular contracture. On the other hand, women with breast implants are able to feel lumps that are smaller in size than their counterparts without implants. This may explain why studies have shown that there is NO difference in the severity or outcome of breast cancer in women with implants compared to women without implants.
In the diagnosis of breast cancer, a procedure called Sentinel Lymph Node Biopsy is used to determine the extent of cancer to direct treatment. This relies on intact lymphatic channels from the breast to the axilla. Although preliminary studies have not shown a problem, any surgery on the breast or axilla theoretically disrupts the lymphatics. New lymphatic channels will form as your body heals if they are divided.
Treatment for breast cancer ranges from breast conservation techniques with or without radiation to complete removal of the breast (mastectomy). Depending on the location of the cancer, you may be able to keep your implants. However, the option of breast conservation may be less likely since your native breast tissue will thin out with time with implants, leaving little tissue to “conserve.” Additionally, if radiation is required, it will distort the shape of your breast and it would be beneficial to have the implants removed. It has been shown that most women with breast implants have a better cosmetic result following a mastectomy with reconstruction as opposed to breast conservation and radiation. Implants used for breast reconstruction are the same as those used in cosmetic procedures.